Cookie Notice
By continuing to use this website, you consent to our use of cookies and the other terms of our Privacy Policy.
For more information, please visit our Privacy Policy.
KENGREAL is administered as a bolus and infusion after reconstitution and dilution.1

Supplied as a sterile, lyophilized powder in 10 mL single-use vials, each containing 50 mg of KENGREAL
Reconstitute the contents of the vial immediately before dilution.
Reconstituted KENGREAL will be a clear, colorless to pale yellow solution. Product should not contain particulate matter.
Do not use reconstituted solution of KENGREAL without dilution.
Dilution can be in either 0.9% sodium chloride injection USP or 5% dextrose injection USP:
Diluted KENGREAL is stable at room temperature for up to 12 hours in 5% dextrose injection and 24 hours in normal saline. Discard any unused portion of reconstituted solution remaining in the vial.
The recommended dosage of KENGREAL is a 30 mcg/kg IV bolus immediately followed by a 4 mcg/kg/min IV infusion. Be sure to administer KENGREAL via a dedicated IV line.1
30 mcg/kg x body weight (kg)
200 mcg/mL

4 mcg/kg/min x 60 min/hr x body weight (kg)
200 mcg/mL
No age-based dose adjustment is required in elderly patients (≥75 years) or for patients with renal or hepatic insufficiency.
To maintain platelet inhibition after discontinuation of KENGREAL infusion, an oral P2Y12 inhibitor should be administered as follows1:
180 mg at any time during KENGREAL infusion or immediately after discontinuation
60 mg immediately after KENGREAL discontinuation*
Do not administer prior to KENGREAL discontinuation
600 mg immediately after KENGREAL discontinuation*
Do not administer prior to KENGREAL discontinuation
*If prasugrel or clopidogrel is administered during KENGREAL infusion, it will have no antiplatelet effect until the next dose is administered.
KENGREAL is an ATP analogue that binds to the same receptor site as ADP
ADP
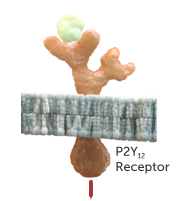
G-Protein
Activation
Thienopyridines (active metabolite): clopidogrel and prasugrel
Signaling
Inhibition
CPTP: ticagrelor

Signaling
Inhibition
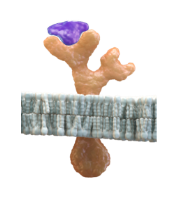
ATP: KENGREAL® (cangrelor)

Signaling
Inhibition
KENGREAL® (cangrelor) molecule blocks active metabolite of thienopyridines binding site

Signaling
Inhibition
CPTP (ticagrelor) is still able to bind to P2Y12 receptor even while KENGREAL is active

Signaling
Inhibition
Reach out to us for more information and updates, or to be contacted by a rep. You can also request resources like dosing and lanyard cards be sent to you.
Consider KENGREAL when treating complex lesions
KENGREAL® (cangrelor) for Injection is contraindicated in patients with significant active bleeding.
KENGREAL® is contraindicated in patients with known hypersensitivity (e.g., anaphylaxis) to cangrelor or any component of the product.
Drugs that inhibit platelet P2Y12 function, including KENGREAL®, increase the risk of bleeding. In CHAMPION PHOENIX, bleeding events of all severities were more common with KENGREAL® than with clopidogrel. Bleeding complications with KENGREAL® were consistent across a variety of clinically important subgroups. Once KENGREAL® is discontinued, there is no antiplatelet effect after an hour.
The most common adverse reaction is bleeding.
KENGREAL® (cangrelor) for Injection is a P2Y12 platelet inhibitor indicated as an adjunct to percutaneous coronary intervention (PCI) to reduce the risk of periprocedural myocardial infarction (MI), repeat coronary revascularization, and stent thrombosis (ST) in patients who have not been treated with a P2Y12 platelet inhibitor and are not being given a glycoprotein IIb/IIIa inhibitor.
Open
Close
